
Tibialis Anterior Tendon Transfer Surgery for Clubfoot
What is Tibialis Anterior?
Tibialis anterior is a strong muscle at the front of the lower leg, that pulls the foot up and in (figure 1). In children with clubfoot, tibialis anterior is often stronger than the muscles on the outer side of the lower leg which pull the foot outwards. This can result in a muscle imbalance which affects the way the child walks.


Figure 2a
Figure 2b
This can be apparent in the front (figure 2a) or back (figure 2b) of the foot.
This is a clubfoot recurrence. If the muscle imbalance persists, the foot can lose flexibility. Ultimately this will lead to pain and dysfunction long term if not addressed.
Tibialis anterior tendon transfer surgery rebalances the muscle forces across the foot. This surgery is globally recommended in cases of recurrent clubfeet. It is part of standard childhood Ponseti clubfoot treatment for recurrent cases. The foot must be sufficiently flexible to have surgery. In cases where the foot has lost flexibility, serial casting over multiple weeks will be required prior to surgery.
What happens during surgery?
With the child asleep under anaesthetic, and through a medium incision, the tendon of tibialis anterior is taken from its insertion on the inside of the foot. One or two more small incisions are made. The tendon is then re-directed and re-attached to the middle of the foot so that muscle balance and function is improved (figure 3)
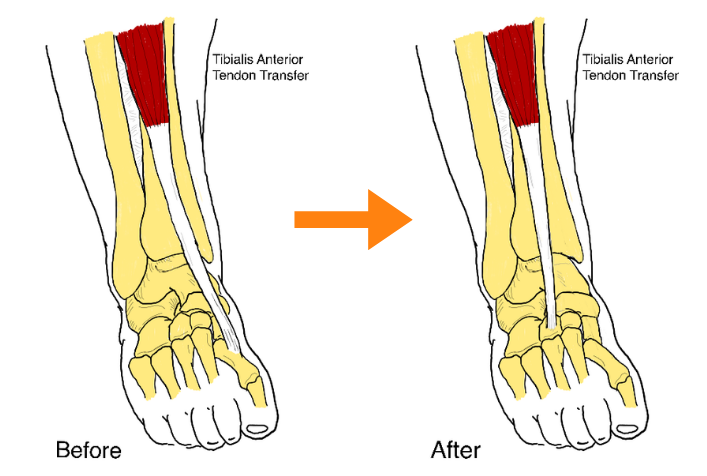
Figure 3
Sometimes other procedures are performed at the same time, such as Achilles tendon lengthening. Numbing medicine is injected into the surgical sites to keep the child comfortable after surgery. Absorbable stitches are typically used for most children. When the surgery is completed, a well-padded below-knee cast is applied to maintain the foot in the corrected position and to allow the tendon to heal into the bone in its new place.
What happens after surgery?
Your child will usually go home on the same day as surgery. Mild swelling is normal. Elevating the leg on pillows is helpful until pain and swelling subside. For most children, Acetaminophen and Ibuprofen are used for pain control after surgery. Acetaminophen (Tylenol) and Ibuprofen (Advil) should be given for the first 48 hours, as directed on the bottle. Some children can experience spasm (a sudden discomfort) in the first few days. You will be given medication at discharge to assist should this occur. The cast must be kept clean and dry. Showering is permitted if the cast can be safely bagged and taped to protect it from water, otherwise sponge-bathe only.

Mobility after surgery
Some children will need a wheelchair for mobility in the community. For the first two weeks, usually no weight bearing is allowed through the affected foot. In some cases the surgeon may allow your child to take a few steps. Children seven years or older may use crutches or a walking frame if only one side has been operated. Younger children will need to be lifted by the parent and will require a wheelchair. Most children do not require suture removal. After two weeks, the child may do limited walking around the house with a cast shoe, which will be given to you at discharge from hospital. The cast will be removed six weeks post-surgery. Some children may require casting for an AFO (ankle-foot orthoses) in Operating Room or clinic, then a new below-knee cast for a further 2-3 weeks. Not all children will be fitted with an AFO.
This information sheet has been adapted for use by families receiving care by clinical members of UBC Orthopedics Division of Pediatric Orthopedics. The information contained in this fact sheet is intended to assist, not replace, discussion with your doctor or health care professional. UBC Orthopedics does not accept any responsibility, and will not be liable for, any inaccuracies, omissions, information perceived as misleading, or the success of any treatment regimen detailed in the fact sheet.
Figure 1
Figure 2a
Figure 2b
