
FOR PARENTS AND FAMILIES: UNDERSTANDING CLUBFOOT
As a parent, you’re not alone in this journey. Clubfoot (also called talipes equinovarus) is one of the most common birth differences, affecting about 1 in 1,000 babies worldwide. Your child’s orthopaedic team will guide you step by step, and your role is essential in guiding the correction and maintaining the correction of your baby’s feet through infancy and childhood.
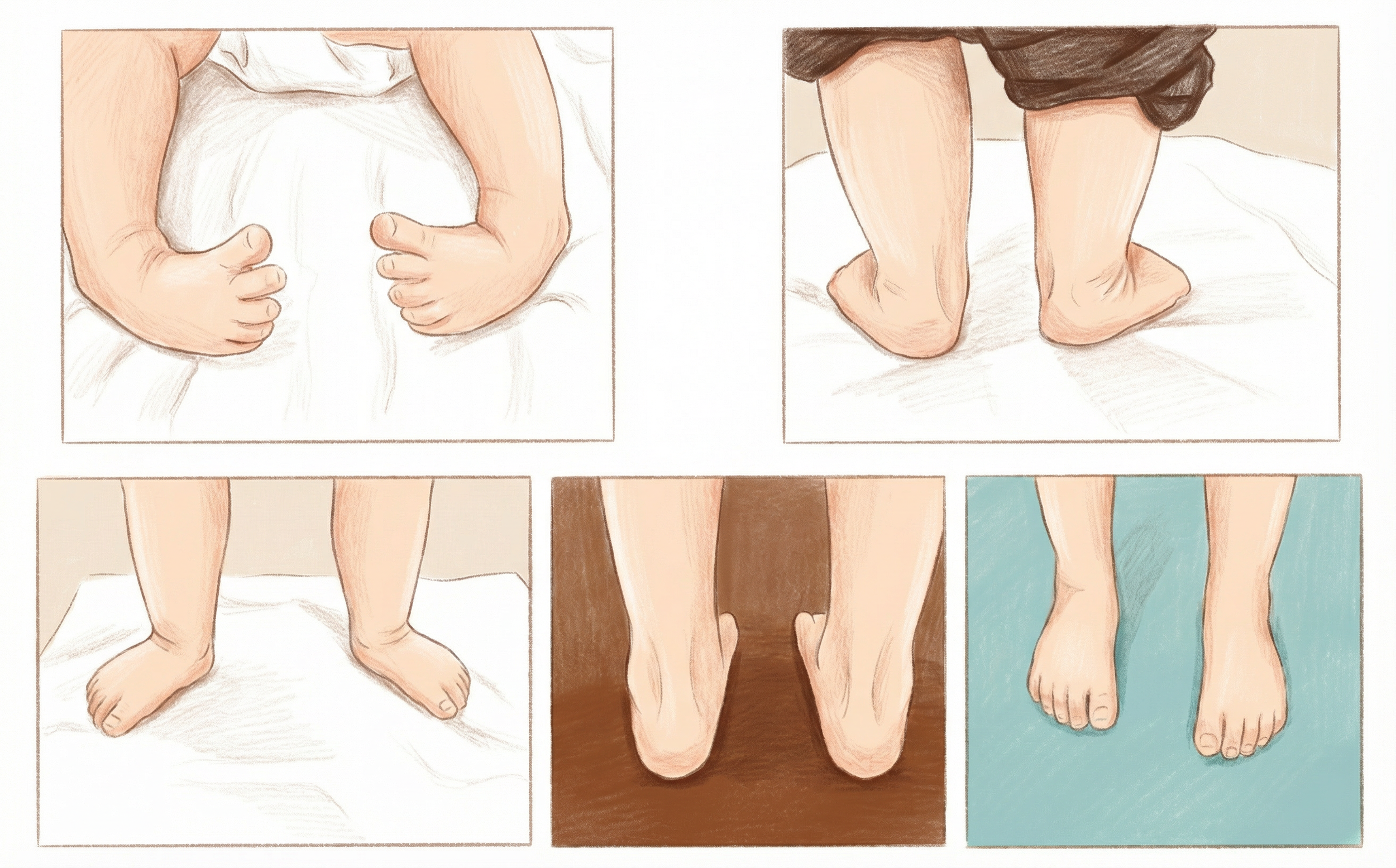
Clubfoot (talipes equinovarus) is a condition present at birth where the foot is turned downward and inward and is rigid (not flexible). All the bones, muscles, and tendons are present, but they are not in the usual alignment. Clubfoot may affect one foot (unilateral) or both (bilateral). It is not painful for babies, and parents should know that it is not their fault. In most cases the exact cause is unknown, although genetics and environment may play a role.
Most cases are idiopathic clubfoot, meaning they occur without other health problems. In some cases, clubfoot may be associated with other conditions and further testing may be recommended.
What is Clubfoot?
Many parents find that once treatment starts, their initial worries are quickly replaced with confidence and optimism as they see their child’s progress.
With early care and maintenance, almost all children born with clubfoot grow up to walk, run, and play just like other kids their age. The standard treatment, called the Ponseti Method, gently corrects the foot with a series of casts, a small procedure on the Achilles tendon, and bracing. This process has an excellent track record: children go on to lead full, active lives, and their feet are usually strong, flexible, and pain-free well into adulthood
Clubfoot is often noticed at birth during a newborn examination, and sometimes detected on prenatal (before birth) ultrasound.
It is a visible condition, where the baby’s foot turns downward and inward appearing shorter around the ankle. This can affect one or both feet. Most babies are otherwise healthy.
Your baby’s doctor or midwife will check:
• The position and flexibility of the foot and ankle
• Whether one or both feet are affected
• If there are any signs of other conditions (for example, muscle weakness or spinal differences)
Your baby will be referred to a clubfoot clinic or orthopaedic surgeon for assessment and treatment.
How is Clubfoot Diagnosed?

What is the treatment?
The Ponseti Method is the gold standard worldwide. It involves three stages:
1. Casting (Correction Phase):
Gentle stretching and weekly casts starting in the first few weeks of life. Typically 5–7 casts are needed.
A minor procedure called a tenotomy is completed in clinic under local anesthetic. This procedure involves cutting the tight Achilles tendon and is often done before the final cast.

2. Bracing (Maintenance Phase):
After the last cast, your baby will wear a boots and bar brace.
Braces are worn 23 hours/day for 3 months, then during naps and nighttime until at least age 4 years
Note: Adherence to bracing protocols is the surest way to prevent recurrence!

3. Monitoring & Exercises:
Parents learn stretching and strengthening exercises to maintain correction. We monitor your child’s progress to assess whether tendon rebalancing is required.
Regular follow-up continues until your child is fully grown.
Tips for Parents
In The Bracing Phase
• Brace wear: Expect fussiness at first!
Babies adapt within days. Always check for red marks or blisters on both feet.
• Play & exercise: Tummy time, squats, and climbing help strengthen the legs.
In The Casting Phase
• Clothing: Loose or snap-up sleepers and pants fit best over casts and braces.
• Bathing: Babies in casts need sponge baths; keep casts dry.
• Diapers: Prevent leaks around casts with snug covers or extra absorbent diapers.
Monitor for signs of Cast Slippage (Count how many toes you see each time you check!), inconsolable crying, toe swelling, skin checks (for red marks or bruising),
Toe colour and blood flow checks (Pressing on a toe should cause it to briefly turn white, then return to pink within 2 seconds. If it takes longer than 2 seconds, try warming up your child’s toes with a warm blanket and comparing to the other side.)